This was enough of a revelation to warrant its own post, plus I include another factor in the limitation of health care we are seeing with COVID-19.
Probably the most important thing to know is that in many cases, your general practitioner does not write the orders for your care while you are in ICU. Orders are written by the “intensivist” who runs that ICU. And so it is noteworthy that COVID wards in the hospitals are designated as ICU wards. Your general practitioner likely has no control over what happens to you in a COVID ward. ICU wards are governed by computer statistical models. There is seemingly no allowance for intuition in the process.
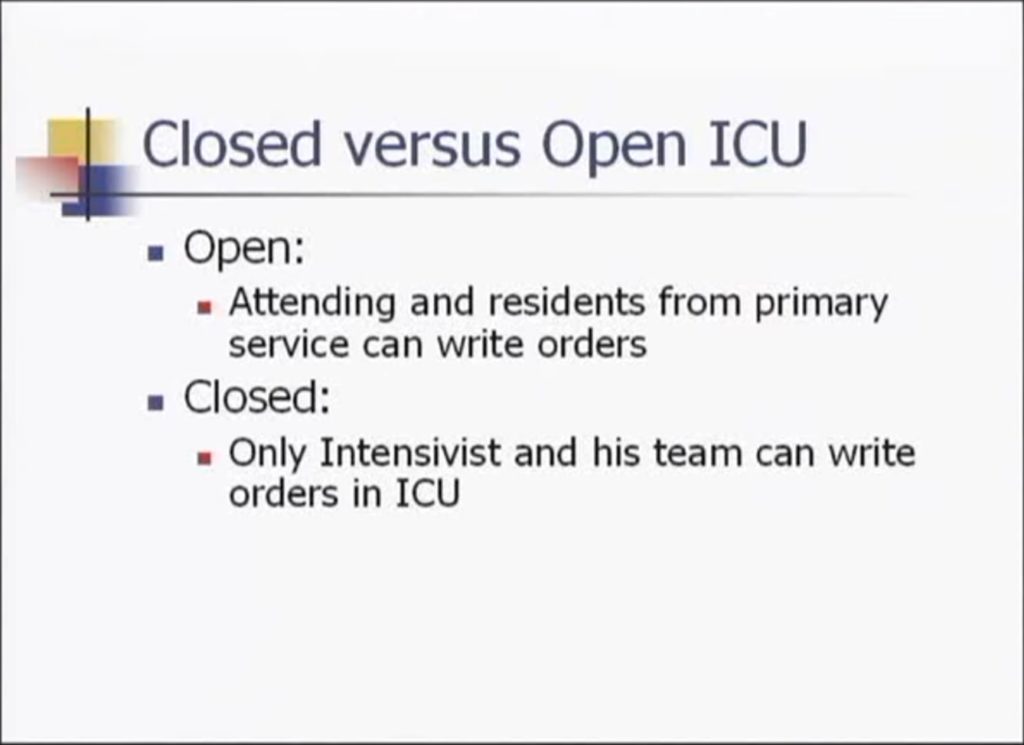
Slide from Dr. Jay Doucet’s presentation
Dr. Jay Doucet claims that closed ICUs have decreased mortality rates, fewer low severity illness admissions, and less frequent complications.
We have come to a place where patients, not their illnesses, are seen as the problem to be solved.
“Patient care” has been replaced by “patient management.”
For critically ill or injured people, the Doctor-patient relationship no longer exists. Individual specialists and surgeons no longer have the final say in patient care, now they are subordinate to a rotating team of critical care ‘doctors’ whose training is mainly in administration, equipment use and statistics.
These teams do not see each person as a unique patient, rather they see an amorphous group of sick people who are draining resources. Their main objective is not to return patients to health, but to ration resources.
These frontline workers are today’s “Trusted Voices” and their stars (and side businesses) keep rising as long as they go along with the approved narratives.
It wasn’t always this way.
— Amazing Polly
A weakness in the intensivist system could exist when the computerized models contain faulty protocols, as we are seeing in COVID-19, and does not allow doctors to stray from that protocol. As they say in computer programming, “Garbage in, garbage out,” often shortened to “GIGO.” This also includes patient data which might be entered incorrectly or not entered at all, such as whether someone has been vaccinated. The current COVID-19 protocol handed down from NIH allows for the use of only Remdesivir and ventilators. No early treatment is recommended. Not only are hydroxychloroquine and ivermectin not on the ICU protocol, but corporate policy often does not allow hospital doctors to prescribe them. This protocol is adhered to so tightly that nutraceuticals are not used, either. That is how we end up with stories such as that of Veronica Wolski and the father of an unknown South Carolina resident who was threatened with arrest when he tried to advocate for his father.
But there may be another issue that is causing these hospitals and intensivists to fail to look at alternative therapies.
At the time of this writing, the Public Health Emergency policy text has already changed. At the time Dr. Robert Malone did the screen print, it said this:
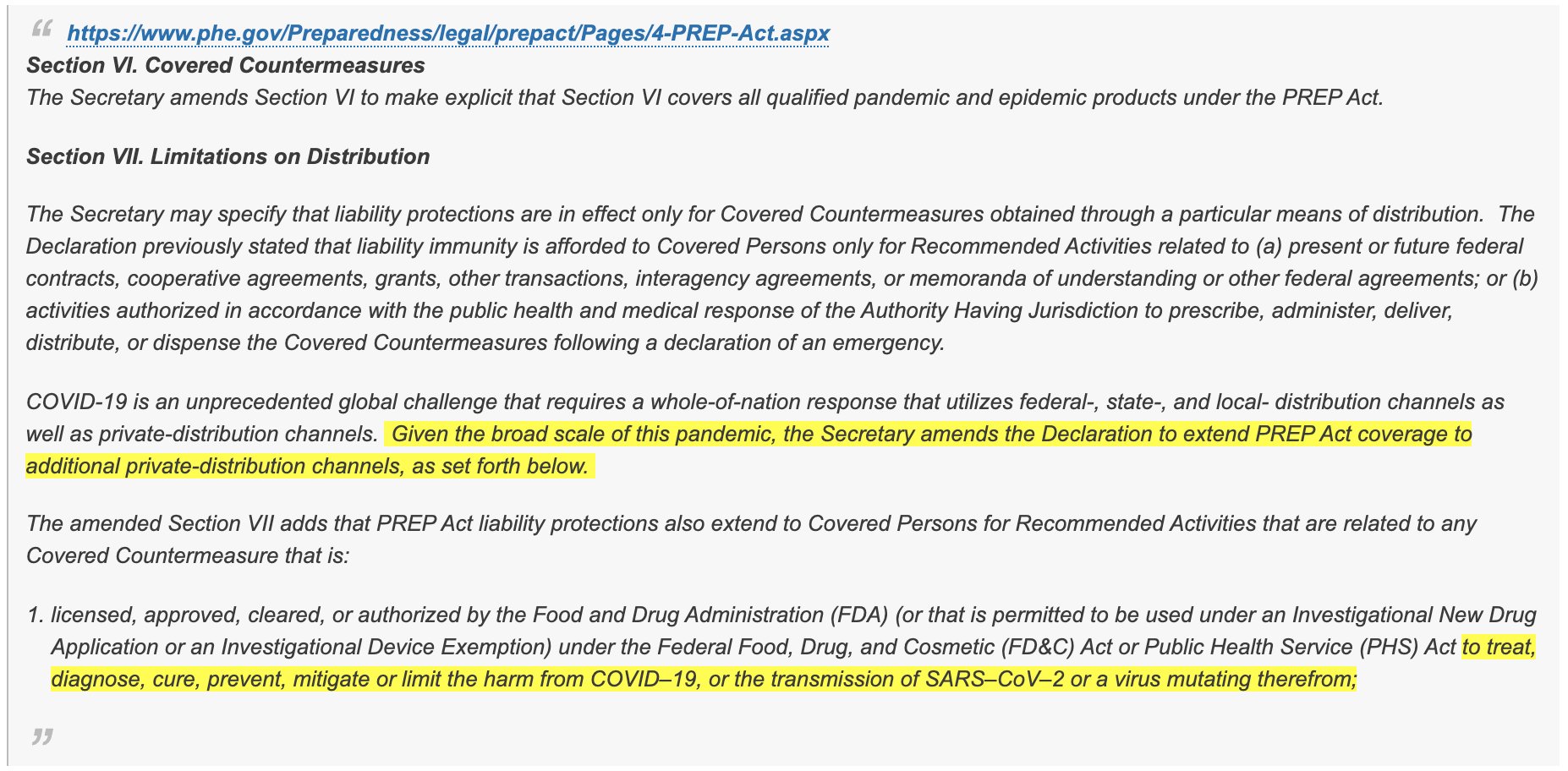
Section VI. Covered Countermeasures
The Secretary amends Section VI to make explicit that Section VI covers all qualified pandemic and epidemic products under the PREP Act.
Section VII. Limitations on Distribution
The Secretary may specify that liability protections are in effect only for Covered Countermeasures obtained through a particular means of distribution. The Declaration previously stated that liability immunity is afforded to Covered Persons only for Recommended Activities related to (a) present or future federal contracts, cooperative agreements, grants, other transactions, interagency agreements, or memoranda of understanding or other federal agreements; or (b) activities authorized in accordance with the public health and medical response of the Authority Having Jurisdiction to prescribe, administer, deliver, distribute, or dispense the Covered Countermeasures following a declaration of an emergency.
COVID-19 is an unprecedented global challenge that requires a whole-of-nation response that utilizes federal-, state-, and local- distribution channels as well as private-distribution channels. Given the broad scale of this pandemic, the Secretary amends the Declaration to extend PREP Act coverage to additional private-distribution channels, as set forth below.
The amended Section VII adds that PREP Act liability protections also extend to Covered Persons for Recommended Activities that are related to any Covered Countermeasure that is:
- licensed, approved, cleared, or authorized by the Food and Drug Administration (FDA) (or that is permitted to be used under an Investigational New Drug Application or an Investigational Device Exemption) under the Federal Food, Drug, and Cosmetic (FD&C) Act or Public Health Service (PHS) Act to treat, diagnose, cure, prevent, mitigate or limit the harm from COVID–19, or the transmission of SARS–CoV–2 or a virus mutating therefrom; or
- a respiratory protective device approved by the National Institute for Occupational Safety and Health (NIOSH) under 42 CFR part 84, or any successor regulations, that the Secretary determines to be a priority for use during a public health emergency declared under section 319 of the PHS Act to prevent, mitigate, or limit the harm from, COVID–19, or the transmission of SARS–CoV–2 or a virus mutating therefrom.
Public Heath Emergency, August 13, 2021
In other words, practitioners are protected from liability as long as they follow the published protocols, and possibly they won’t get paid if they don’t.
In the cases of Veronica Wolski and the father of an unknown South Carolina resident, they were both in the hospital long enough that it should have been clear that these patients were not thriving on the care that was being given. And yet there was no flexibility in the policies followed in the hospitals to allow them to try alternative treatments such as hydroxychloroquine or ivermectin in spite of the efforts of advocates for the patients for something else to be tried.
When a patient’s health continues to decline on the standard protocol, is it not the responsibility of the doctor to try a different protocol when asked, especially when others have reported great success with that protocol? Does the protection of the PREP Act shield doctors and hospitals from murder charges when hospital administrators willfully refuse to discharge a patient to the care of another provider upon request from the patient or someone holding power of attorney?
Remember: “I was just following orders” did not help those on trial at Nuremburg.
Sources:
- September 17, 2021. How Hospitals Are Killing Us – Many BOOMS! Amazing Polly. Runtime: 1:23:52.

https://www.bitchute.com/video/Fam1bTnPB9LO/.
Video. - May 19, 2012. Jay Doucet. Who’s in Charge in the ICU. UCSDTraumaBurn. Runtime: 11:30.

https://www.youtube.com/watch?v=iPsZ_XuiSes.
Video, Expert. - September 15, 2021. Unknown South Carolina resident. South Carolina Senate Medical Affairs Committee 9/15/2021. Will Folks.
https://www.youtube.com/watch?v=2sT5yzJ1voY.
Video. - August 31, 2021. Robert W Malone. “Thread by @RWMaloneMD on Thread Reader App.” Thread Reader App.

https://threadreaderapp.com/thread/1432782568382939139.html.
Social Media, Expert. - Alex M. Azar II. “Fourth Amendment to the Declaration Under the Public Readiness and Emergency Preparedness Act for Medical Countermeasures Against COVID–19 and Republication of the Declaration.” Public Heath Emergency. Accessed August 13, 2021.

https://web.archive.org/web/20210813193727/https://www.phe.gov/Preparedness/legal/prepact/Pages/4-PREP-Act.aspx.
Government. - Alex M. Azar II. “Fourth Amendment to the Declaration Under the Public Readiness and Emergency Preparedness Act for Medical Countermeasures Against COVID–19 and Republication of the Declaration.” Public Heath Emergency. Current version.
https://www.phe.gov/Preparedness/legal/prepact/Pages/4-PREP-Act.aspx.
Government. - August 26, 2021. Peter McCullough. Dr Peter McCullough Lecture on the State of COVID Treatment. DoctorTed.
https://rumble.com/vlqdpo-dr-peter-mccullough-lecture-on-the-state-of-covid-treatment..html.
Video, Expert. - June 3, 2008. Mitchell M. Levy, John Rapoport, Stanley Lemeshow, Donald B. Chalfin, Gary Phillips, and Marion Danis. “Association between Critical Care Physician Management and Patient Mortality in the Intensive Care Unit.” Annals of Internal Medicine 148 (11): 801–9.

https://doi.org/10.7326/0003-4819-148-11-200806030-00002.
Research Journal.
“Patients who received critical care management (CCM) were generally sicker, received more procedures, and had higher hospital mortality rates than those who did not receive CCM.”
Related:
- September 22, 2021. Hospital Insiders Reveal Soulless COVID Protocols. MorePolly. Runtime: 28:12.
https://www.bitchute.com/video/pNV2AUkrf6ev/.
Video. - September 3, 2021. HOW NOT TO BE MURDERED BY THE PROTOCOLS — Robert Beadles. SGT Report. Runtime: 50:35.
https://www.bitchute.com/video/myTa8hAnTUO2/.
Video. - September 19, 2021. David Whited and Stacy Whited with Bryan Ardis. What Is More Dangerous? (COVID-19 or the COVID-19 Hospital Protocols?). Thrivetime Show: Business School without the BS. Runtime: 1:42:57.
https://rumble.com/vmp4pz-what-is-more-dangerous-covid-19-or-the-covid-19-hospital-protocols.html.
Video, Expert. - “Corruption of Health Regulatory Organizations, Big Pharma, and Media.” Compilation of Scientific and Medical Research, Data, & Reports.

http://www.kathydopp.info/COVIDinfo/Vaccines/HealthAgencyPharmaCorruption.
Reference. - June 3, 2022. Sarah Westall with Daniel Satchkov. AI Is a LIE, But It Is Dangerous to Humanity w/ Daniel Satchkov. Sarah Westall – Business Game Changers. Runtime: 13:05.
https://www.bitchute.com/video/mIPKWF8Hm8zx/.
Video.
The computerized systems cut God out of the equation. In fact, they force God out. There is no room for doctors who are caring for failing patients to pray and receive an answer about what the patients need. Those doctors would not be free to implement the answers they had received unless the computer model already included them. This was the crime, even if not necessarily a crime of this earth — the forcing of God out. Doctors in these systems are no longer allowed to act on their intuition. There is no point in praying when working within these computerized systems. Doctors cannot be creative when working within these systems. The computerized systems and those who work within them assume that all is known. Survival rates can only falter in a pessimistic computerized system based entirely on statistics. Without an allowance for new methods, experience, and knowledge that has been normal in medicine, cases that do not fit existing models are more likely to fail, dragging down the statistics as these intensivists do not offer hope for a solution. These computerized systems can suck the hope out of people, just as Satan and his minions do. I wonder what those with spiritual sight would see in one of these computerized ICUs…
Furthermore, policies specific to COVID-19 have blocked avenues normally available to doctors, such as the off-label use of medicines. God needs to be restored to His place in medicine, and doctors need to be restored to their role as creative problem solver without hinderances that interfere in their intuitive processes.